Outsmarting the Deadliest Brain Cancer
Northwestern scientists are testing novel approaches to break the grip of glioblastoma. By Clare Milliken
Image: Illustration by Daniel Zender
Author’s note: We are honored that Ned Smith was willing to share his story with us earlier this year. Unfortunately, Ned's tumor recurred during the summer, and he transitioned to hospice care in September. He passed away on Sept. 25, 2021. Our thoughts are with his family, friends, colleagues and everyone who knew and loved him.
Three years ago, Ned Smith was shopping with his youngest daughter, Cecily, and his wife, Erin. Smith, then 38, had his daughter on his shoulders when he tripped and fell on the sidewalk. Erin insisted they go to the hospital. Her husband had been tired and off balance for a week, and now it was time to investigate.
After several scans and tests, Smith was diagnosed with glioblastoma, the most prevalent, hardest to treat and deadliest of all cancers that begin in the brain.
About 25% of patients with glioblastoma survive two years after their diagnosis. Fewer than 5% survive five years, and fewer than 1% survive 10 years. And those years and months of survival can be brutal — filled with treatment side effects and impairments to speech, cognition, sight, movement and more.
For Smith, his life as a father of four, a husband and an associate professor in the Kellogg School of Management was suddenly interrupted by cycles of radiation and chemotherapy. A social scientist, Smith pored over glioblastoma research studies as the left side of his body went numb. He suffered seizures and devastating fatigue. He spent months in a wheelchair and lost his sense of time.
“Glioblastoma goes to the heart of who we are. It grabs you at the soul,” says Maciej Lesniak, the Michael J. Marchese Professor of Neurosurgery and chair of neurological surgery at the Feinberg School of Medicine. “Our whole entity — who we are as human beings — is focused on our central nervous system, and this is a cancer that basically liquefies your brain and destroys it.”

Ned Smith with his wife, Erin, their four children and the family dog. Credit: AFMPHOTO
At Northwestern, Lesniak and others have spent decades searching for answers to a vexing cancer. From bench to bedside, these scientists have shed new light on glioblastoma, brought new technologies to patients and even developed promising therapies that could revolutionize glioblastoma treatment — and cancer care more broadly. “It’s a field [ripe] for new advances,” says Lesniak, who is also program leader in neuro-oncology at the Robert H. Lurie Comprehensive Cancer Center of Northwestern University. “There is a lot of opportunity here to make a dent in the disease.”
“Early in my career, I would give the diagnosis, and the first question [a patient asked] would be, ‘What’s the prognosis?’” says James Chandler, the Lavin/Fates Professor of Neurological Surgery and vice chair for clinical affairs in the neurological surgery department at Feinberg. “I would go into an explanation about survival curves, and then I had patients who survived five years and 10 years. And I realized everybody’s different, there are new advances every year, and the worst thing that you can do is to strip a patient and their family of hope.”
An Insidious Beast
Glioblastoma is a fast-growing tumor that spreads easily throughout the brain. There are treatments for the initial “primary” tumor, but the cancer survives and grows in nearly all instances, and treatments for recurrent tumors only add months of survival at best. “Remission doesn’t apply to glioblastoma,” Smith says. “The cure rate is essentially zero.”
Newly diagnosed patients typically undergo surgery to remove as much of the tumor as possible. But even that has its limits.
“By the time a patient has symptoms that would cause them to go for a neurological exam, the tumor has existed long enough that its cells have disseminated to near and far regions of the brain,” says C. David James, professor emeritus of neurological surgery at Feinberg.
Surgery cannot remove all traces of the tumor because glioblastoma spreads throughout the brain. “In other words, what we see on the scan is only the tip of the iceberg,” says Roger Stupp, chief of neuro-oncology and the Paul C. Bucy Professor of Neurological Surgery at Feinberg. “Even the best-skilled surgeon cannot get every last cell.”
The variation of these tumor cells is another critical roadblock. “At a cellular level, the tumor is made up of many different subpopulations of cells, which provides it with an incredible ability to survive,” James says.
“[Glioblastoma] grows really fast, and it’s smart — that’s the headline,” says Priya Kumthekar ’08 GME, ’11 GME, ’12 GME, associate professor of neurology and medicine at Feinberg. “It can change its genetic composition over time and in response to treatment. It can be treated and sit still for six or nine months, and then suddenly it will grow over a three- or four-week period.”
Roger Stupp, left, and James Chandler, co-directors of the Northwestern Medicine Lou and Jean Malnati Brain Tumor Institute of the Robert H. Lurie Comprehensive Cancer Center of Northwestern University. Credit: Michael Parra
The tumor’s location in the body also poses challenges.
“The brain is our most delicate organ,” Stupp says. “It’s one of the few organs that is not duplicated. I can take out half of the lungs, but I cannot take out half of the brain.”
The organ is also surrounded by the blood-brain barrier, an ordinarily protective structure that, in the treatment of glioblastoma and other brain tumors, hampers success.
“The blood-brain barrier prevents substances from getting into the brain,” Lesniak says, “and it presents some practical difficulties for us to achieve things that are easier to do with systemic cancers [like breast or colon cancer].”

Illustration by Daniel Zender
Zapping Tumors
Stupp, one of the world’s leading neuro-oncologists, is committed to thinking unconventionally about treating glioblastoma. In the early 2000s he found that the combination of radiation and the chemotherapy drug temozolomide extended the lives of some glioblastoma patients.
With this treatment, the number of glioblastoma patients surviving two years grew from 1 in 10 to 1 in 4. Known today as the Stupp protocol, the combination of radiation and temozolomide has been the standard for newly diagnosed glioblastoma patients since 2005.
Stupp’s outside-the-box thinking didn’t stop there. He began working on a device that uses pulses of electricity to interfere with cancer cell division and ultimately kill cancer cells. The tumor-treating fields (TTFields) device consists of 36 electrodes placed on the patient’s shaved head. Powered by a 3-pound portable battery, the device is worn continuously. Patients don’t feel the pulses at all, and the side effects are relatively minor.
In a clinical trial of almost 700 patients with glioblastoma, those who wore the device while also receiving standard radiation and chemotherapy treatment survived a median of 20.9 months, compared with 16 months for patients who did not use the device. Forty-three percent of patients using radiation and temozolomide plus the TTFields device survived two years.
Ned Smith received radiation and temozolomide. He wore the TTFields device until he became eligible for a clinical trial of a personalized cancer vaccine in Germany.
“When I was waiting to get started in Germany, I didn’t know if I would make it to that point,” says Smith. “I committed to myself and my family that I would keep the device on until I got to Germany.”
Tumor-Eating Viruses
One Northwestern team is studying a treatment that uses viruses to destroy tumors. The investigational treatment leverages an oncolytic virus, which is capable of infecting — and potentially destroying — brain cancer cells.
Previous research using this approach has shown the virus struggles to permeate the entire tumor. But Lesniak’s team decided to go in a new direction — becoming the first in the world to use neural stem cells to deliver a virus to the tumor.
“Neural stem cells have been shown in many preclinical and clinical models to be almost like little cars,” Lesniak says. “Once you inject them, they will actually travel throughout tumor masses.”
The treatment, Lesniak says, works like this: During the initial surgery to remove as much of the tumor as possible, the virus-loaded neural stem cells are injected into the brain cavity. The virus has been genetically modified to bind to a protein expressed on the surface of glioblastoma cells. When it recognizes that protein, the virus will infect the cancer cell, replicate within it and ultimately kill the cancer cell.
“Think of this as the missile and warhead of an atomic bomb,” Lesniak says. “There’s a missile that delivers the nuclear warhead. The stem cells are the missile, and the virus is the warhead.”
But unlike an atomic bomb that levels everything indiscriminately, the virus leaves healthy cells unscathed.
Lesniak, who is principal investigator of the virus project, co-directs a five-year, $11.5 million Specialized Program of Research Excellence grant from the National Cancer Institute. The grant was awarded in 2018 in recognition of the Lurie Cancer Center’s leadership in glioblastoma treatment research.
In a Phase I trial, Lesniak’s team found the virus treatment to be safe and, in some patients, superior to the standard of care. Lesniak cautions, though, that further study is needed. If subsequent results are positive and the treatment is approved by the Food and Drug Administration, oncolytic virotherapy could offer a new treatment for primary glioblastoma tumors.
“Many of the clinical trials that we do for glioblastoma are at the time of recurrence,” Lesniak says. “So patients get standard of care, and then when the cancer recurs, the patient signs up for experimental therapies. [But] in this upfront setting, patients would have surgery to remove the tumor followed by an injection of this product and then standard of care. The FDA allowed us to do [this study] in newly diagnosed patients, which hasn’t been done before.”

Priya Kumthekar, right, and Karan Dixit review data in a clinic.
Image: MICHAEL PARRA
Spherical Nucleic Acid Therapy
Other Northwestern researchers are exploring novel ways to deliver treatments across the blood-brain barrier. Associate professor of neurology and medicine Alexander Stegh is using nanotechnology to penetrate the barrier and target genes implicated in the disease.
Alexander Stegh, right, works in a lab. Credit: Robert Knapp
During his postdoctoral work at the Dana-Farber Cancer Institute and Harvard Medical School, Stegh was part of a team that discovered the Bcl2L12 gene was significantly overexpressed in glioblastoma and contributed to treatment resistance. By dialing down the expression of the gene, the team reasoned, treatments could be more effective. But conventional therapies cannot target Bcl2L12, Stegh says, necessitating a novel means of drug development and delivery.
At Northwestern, Stegh partnered with Kumthekar and Chad Mirkin, the George B. Rathmann Professor of Chemistry and inventor of spherical nucleic acids (SNAs). These tiny three-dimensional structures are composed of a nanoparticle core that can be surrounded by RNA or DNA strands. These strands can be selected to target, and dial down, the expression of certain genes. The structure of SNAs offers unique drug delivery benefits as well.

Chad Mirkin meets with his team. Credit: Joel Wintermantle
“SNAs, unlike normal DNA and RNA, are naturally taken up by cells,” says Mirkin, who is also the director of Northwestern’s International Institute for Nanotechnology. “Once you get large amounts of DNA and RNA into cells, you think, ‘Wait a second. We could use SNAs as a drug. We could use SNAs to regulate what goes on in cells.’”
In a 2013 study, Mirkin, Stegh and others sought to do just that, injecting SNAs programmed to target Bcl2L12 into mice with glioblastoma. The nanoparticles did what the researchers had hoped, crossing the blood-brain barrier, regulating Bcl2L12 and slowing glioblastoma progression.
“We could actually see that these particles accumulated at very high levels within the glioblastoma tumor,” Stegh says. “And we showed that they actually dial down the expression of cancer-causing genes within the tumor. Based on these studies, we could also show that they can slow down tumor progression.”
Just this year, a subsequent study with glioblastoma patients reported equally impressive results. Patient tumors treated with SNAs expressed markers of tumor cell death, compared with those in patients who did not receive the SNA treatment. These effects were seen even though the researchers were required to use a tiny dose of the treatment — just 1/50 of the dose patients would receive in a clinic if the treatment were approved.
“Imagine if you took a Tylenol at a fraction of the strength of the normal dose and it got rid of your headache,” says Kumthekar, who was the principal investigator of the clinical trial. “You’d think, ‘Wow, we have something here.’”
Stegh aims to investigate whether SNA-based gene therapy, combined with radiation and temozolomide, can amplify the effect of the therapy. Meanwhile, this research goes beyond Bcl2L12.
“This is a study that tells you that we could go after lots of different genes,” Mirkin says. “We now know SNAs are well tolerated and they can cross the blood-brain barrier, localize in tumors and hit their target. This allows us to take many shots on goal until we get the right therapeutic or right combination of therapeutics to give us the result we want.”
The recent advances in glioblastoma research across Northwestern have been remarkable, says Leonidas Platanias, the Jesse, Sara, Andrew, Abigail, Benjamin and Elizabeth Lurie Professor of Oncology at Feinberg and director of the Lurie Cancer Center. “The science behind these discoveries will help our patients for generations to come.”
Those discoveries cannot come soon enough for the thousands of people diagnosed with glioblastoma each year who keep parenting, working and living with this deadly disease.
Clare Milliken is senior writer and producer in Northwestern’s Office of Global Marketing and Communications.
Editor’s note: Chad Mirkin and Alexander Stegh have financial interests in Exicure. Northwestern University also has financial interests in Exicure and intellectual property interests in technologies discussed in this article.
{kind=link}
Check out these related stories...
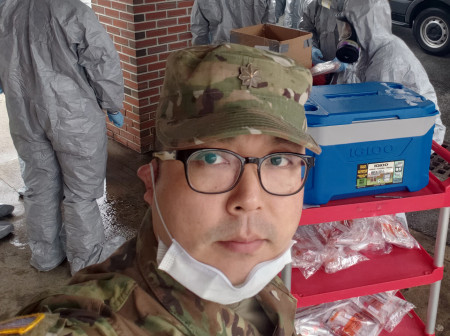
A Sense of Duty and Community
For the past month, Ryan Lee has been leading 18 Massachusetts Army National Guard strike teams, coordinating COVID-19 testing for some of the state’s most at-risk residents. Lee, a dental officer providing medical supervision and quality control, has helped train 225 soldiers who have administered more than 9,000 tests in nursing homes, hospitals, veterans’ homeless shelters and mental health facilities.
Hearing Aides
Last August, Northwestern audiology graduate students made the trek to Nuevo Progreso in western Guatemala to provide comprehensive care for the local residents. Over the course of four more-than-12-hour days, eight students worked alongside four professional audiologists to perform diagnostic testing and hearing-aid fittings.

Reader Responses
I was diagnosed 12 months ago at U of Iowa Hospitals, Dr. Morgan and a very successful resection by Dr. Zanati. Chemo and radiation that went well enough according to December and February scans. Next MRI at UofI in April will be used to consider Gama Knife Radiation for new tumor, and Bcl2L12, SNA. GOD WILLING.
Thanks to all you great medical professionals, thanks to all our caregivers, prayers for all that walk this path, love and peace to each of you.
—Mike Martin Dubuque, Iowa
We are in the fight of our life now, racing against time and trying new procedures to fight GBM. So far it's like Whack-a-Mole. Surgery, gamma tiles, radiation, chemo, and three more tumors show up. Never a clean MRI. Hope, fight, pray, cry, money, strangle our daily lives living and watching our loved one decline. God bless those still fighting this devastating disease, and may your team of doctors get the right combination of therapy for you.
—Holly Reynolds '65, Scottsdale, Ariz.
My wife lived for three years after she was diagnosed with glio. I prayed and prayed for a miracle, but the tumor came back. She was a fighter, as I was her caregiver and watched her take her last breath. That was so hard. Thank you, Northwestern, for giving patients hope to beat this tumor. I pray you succeed in beating this dreaded disease. God bless.
—James Dolr Gahanna, Ohio
Great article! Great science writing, in plain English, without "science-y" jargon at the expense of clarity, and with thoughtful commentary on the human toll of this disease. Clare Milliken seems really to have understood the topic — it's very hard to write so simply and elegantly otherwise. Kudos.
And condolences to Ned Smith's family. What a brave man to share his experience in the face of such a devastating disease.
—Heather Collins '91 MBA, Evanston, via Northwestern Magazine
No one has commented on this page yet.
Submit a Response